

Do you think azithromycin or doxycycline administered daily to frontline NHS workers prevent them from developing COVID-19? Researchers from the University of Salford tell us more.
Hope has been raised for NHS workers as a potential treatment for the corona virus may be on the horizon. Professor Michael P Lisanti and colleagues from the University of Salford, UK, are proposing a new mechanistic framework for understanding how ageing and senescence could contribute to the lethality of COVID-19 in older patients, suggesting the use of anti-ageing drugs as a new clinical approach. Many of these MHRA/FDA-approved drugs are antibiotics, such as doxycycline and azithromycin, which strongly inhibit both inflammation and viral replication, by blocking protein synthesis as a side effect.
A cost of as little as 10p per patient per day
“We have identified several classes of existing MHRA/FDA-approved drugs that, we believe, will help to target the COVID-19 corona virus, for both preventing and treating the disease and at a very low cost to the NHS,” according to lead author Professor Lisanti.

Professor Lisanti is the Chair of Translational Medicine at the University of Salford; and his laboratory has previously published groundbreaking work on the molecular basis of normal ageing, called cellular senescence, and how removing senescent cells with ‘senolytic’ drugs could prevent and possibly reverse ageing-associated diseases.
Interestingly, his latest commentary article discusses how senescent cells may be the key to understanding how to treat COVID-19 infections, with MHRA/FDA-approved drugs. Professor Lisanti and his team propose that these drugs could be effective and would be readily available, with a cost of as little as 10 pence per patient per day.
Azithromycin treating COVID-19 infections
One of the proposed drugs is the antibiotic azithromycin, which is widely used to treat chest, sinus, throat and skin infections, as well as sexually transmitted diseases.
Professor Lisanti adds: “Azithromycin is known to stop the production of cytokines, a torrent of inflammatory mediators that trigger life-threatening lung inflammation in corona virus patients; azithromycin has also been shown to block the production of other viruses, such as the Zika and Ebola viruses”.
In combination with hydroxychloroquine, azithromycin was recently shown to inhibit the replication of the COVID-19 corona virus, in a clinical trial in France. However, the effects of azithromycin alone were not assessed.
Senescence and COVID-19
Looking at the host receptors of COVID-19, they are related to senescence. Two proteins have been proposed to be the cellular receptors of COVID-19: one is CD26 – a marker of senescence, and the other, ACE-2, is also associated with senescence. Therefore, older people would be predicted to be more susceptible to COVID-19, exactly as is observed clinically in patients. This could increase their probability of infection, and would explain the increased fatality of COVID-19 infection in older patients. All of this could be related to advanced chronological age and senescent cells.
Professor Lisanti explains: “If that is the case, then we could intervene, by targeting and removing senescent cells or by using other classes of anti-ageing drugs, to reduce the serious inflammatory reaction caused by the SASP (senescence-associated secretory phenotype). This has the potential to prevent COVID-19 transmission and to ameliorate the associated life-threatening symptoms.”
So how do you remove senescent cells? By administering senolytic drugs, many of which are existing FDA/MHRA approved drugs. Azithromycin is FDA/MHRA approved, and it is used mainly for lung infections, but the Lisanti laboratory found that it selectively targets and removes 97% of the senescent cells.
Vaccines could be 18 to 24 months away, so it would be necessary to identify MHRA/FDA approved drug candidates to repurpose for the prevention and treatment of COVID-19 disease, while we wait.
Now, we need to put these drugs into clinical trials. They are already considered safe, as they have passed Phase 1 clinical trials, so we have absolutely nothing to lose.
Watch the full interview below:
We need to put these drugs into clinical trials
One of the first clinical studies published in the Lancet, showed that COVID-19 infections were most lethal in patients with advanced age, or ageing-associated diseases (diabetes and heart disease), with an elevation of IL-6, a key marker of senescence-associated inflammation.
Clinically, it appears what is leading to fatalities in older patients is the very strong inflammatory reaction and the resulting fibrosis. Azithromycin inhibits inflammation-induced fibrosis, by targeting and removing senescent cells. The cost would be minimal, as the drug is off-patent, widely available and considered safe.
Other senescence-related and anti-ageing drugs, such rapamycin, doxycycline, and hydroxychloroquine could be made available, with support of the relevant regulatory authorities.
For example, in the United States, FDA-approved drugs can be medically prescribed for an ‘off-label’ use, at the discretion of the practising physician.
Unfortunately, the longer we wait, the more people will die. There are not enough respirators, so we need to do something innovative, with great urgency.
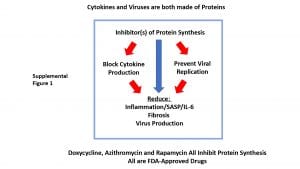
Inhibitor(s) of protein synthesis block inflammation and viral replication. Mechanistically, this is because cytokines and viruses are both made of proteins. Both use the cellular ribosomes for protein synthesis. Inhibiting virus production should help to clinically reduce viral transmission to other patients.



















Please note that doxycycline has in silico action against SARS-CoV-2 proteases. In one study looking at computational screening it had the same strong interaction as remdesivir. Doxycycline is already being used in combination with hydroxychloroquine in Michigan and Long Island.
The point I’m trying to make is that there is nothing to lose by trialling whether doxycycline will help prevent worse cases of COVID-19.
Most severe cases involve the elderly, with co-morbid conditions, which I’m sure are cardiovascularly related, therefore doxycycline would seem more cost-effective, safe and less likely to spread antibiotic resistance.
Doxycycline has been shown to decrease IL-6, TNF alpha levels during dengue infections.
The use of doxycycline as a potential prophylaxis treatment for COVID-19 may be warranted. Doxycyline
inhibits metalloproteinases (MMPs), an group of enzymes implicated in acute respiratory distress
syndrome (ARDS), a major complication of COVID-19.(1)
Papain-like proteinase (PLpro) is responsible for proteolytic cleavage of the replicase polyprotein to
release non-structural proteins 1, 2 & 3 (Nsp1, Nsp2 and Nsp3) which is essential for viral replication.(3)
Virtual ligand screening of potential drug targets of SARS-CoV-2 showed that doxycycline ranked 6th as
potential PLpro inhibitor.(3) Ribavirin ranked 1st overall for relative binding affinity.(3)
3C-like main protease (3CLpro) or Nsp5 which is cleaved from the polyproteins causes further cleavage
of Nsp4-16 and mediates maturation of Nsps which is essential in the virus lifecycle.(3) Virtual ligand
screening showed doxycycline had high binding affinity to 3CLpro, ranking 26th overall.(3)
Doxycycline is an ionophore (forms complexes to facilitate cell membrane transport) and binds divalent
cations (including Zn2+).(4) Zinc has an inhibitory effect on the replication on SAR-CoV.(5) Zinc inhibits
proper processing of replicase proteins and RNA dependent RNA polymerase (RdRp) activity.(5)There
is a strong case for use of a zinc supplement in combination with doxycycline as an antiviral
chemotherapy.(5)
Therefore, doxycycline administered at a high dose of 100mg twice daily to healthcare workers or other
patients at high risk, with a high dose zinc supplement, preferably administered 4 hours apart from the
doxycycline dose to allow absorption (and prevent GI chelation), may be considered. The relatively
benign side effect profile and affordability of this regimen would further support its use.
My message is as a patient so this is probably not the right forum for this comment but if it helps in your trials please feel free to contact me. I started with symptoms of the virus on Sunday, by Monday I was struggling to breath, breathless when trying to speak, pain in my upper chest,coughing, lethargic, gastric issues etc. I initially contact my GP as the coughing was raising my intercranial pressure (i have IIH) and I also have Lupus SLE And Sjögrens. I have already been taking hydroxychloroquine for 2 years for my lupus. GP prescribed doxycycline of which I am on day 4 of the treatment, my symptoms have pretty much disappeared! I can breathe freely, no chest pain, cough almost gone too. I suffered minimal side affects (head ache). Keep up your amazing work!