
Professor John A. Kanis, Honorary President of the International Osteoporosis Foundation and lead author of ‘SCOPE 2021: a new scorecard for osteoporosis in Europe’ discusses the new report which reveals the immense burden of osteoporosis and compares service provision and uptake across Europe.
In 2019, an estimated 32 million people aged over 50 in Europe were diagnosed with osteoporosis (5.6% of the total European population). The condition, which is characterised by bones becoming progressively fragile and even breaking, can often go undiagnosed until a fracture occurs. Despite the health economic burden associated with osteoporosis, fracture prevention strategies and post-fracture care services are lacking. Last year, the International Osteoporosis Foundation (IOF) released a Scorecard for Osteoporosis in Europe (SCOPE) report highlighting the disparities and inadequacies in osteoporosis care across the 27 member states of the European Union, the UK and Switzerland. To find out more, HEQ spoke to lead author and IOF Honorary President Professor John A. Kanis.
Can you tell us a bit about the Scorecard for Osteoporosis in Europe (SCOPE) project and its overall aims?
The Scorecard for Osteoporosis in Europe (SCOPE) project, published under the auspices of the International Osteoporosis Foundation (IOF), aims to raise awareness of osteoporosis burden and care in Europe. It allows for an in-depth comparison of the quality of care for osteoporosis across the 27 member states of the European Union (EU27), together with the UK and Switzerland (termed EU27+2).
SCOPE summarises key indicators of osteoporosis that could be applied to each of the 29 European countries under four broad domains: burden of disease, policy framework, service provision, and service uptake. The Scorecard also draws attention to the disparities in healthcare provision and reviews and compares the previous SCOPE data from 2010 to data as recent as 2019. This allows us to compare and benchmark progress in the management of osteoporosis over time, within and between the EU27+2 countries.
Osteoporosis is a complex, chronic disease that in the EU27+2 results in an estimated 4.3 million fragility fractures annually – or 11,705 fractures per day – causing pain, disability, reduced mobility in individuals. Nevertheless, despite improvements in medication and diagnostic techniques over the past 30 years, osteoporosis remains vastly underdiagnosed and undertreated. Out of €56.9 billion of total direct costs paid in 2019 for fragility fractures, €36.3 billion were spent for direct costs of incident fractures and €19.0 billion for ongoing long-term disability costs from fractures that occurred before 2019. Yet only 3% is spent on medical treatment to prevent recurring fractures.
Through SCOPE we aim to stimulate a common and optimal approach to managing osteoporosis throughout Europe, setting a pathway to improved patient care and fragility fracture prevention.
Why do you think there are such disparities in fracture risk prevention and osteoporosis care across Europe?
In comparison to other regions of the world, European populations are either moderate or high in terms of hip fracture risk. The probability of future hip fracture in men and women at the age of 50 varies enormously, from 3.8-10.9% in men and 7.0-25.1% in women. Women in Sweden have a nearly three-fold greater hip fracture rate (730 per 100,000) compared to women in Romania (246 per 100,000). The reasons for the variation in fracture risk between countries are speculative, but studies have shown weak, but significant, relations between hip fracture risk and latitude, and socio-economic prosperity.
Disparities in service provision and care for osteoporosis can be attributed to a number of factors. Healthcare spending as a percentage of GDP in the EU varies enormously, from 11.3% in France to 5.2% in Romania. The degree to which musculoskeletal health is prioritised also varies: our audit of national osteoporosis societies in 2020 found that governments recognise osteoporosis or musculoskeletal diseases as a national health priority in only nine of the 28 European countries which responded to the survey.
Treatment pathways also vary across Europe. The majority of patients are preferably managed in the long-term at the primary healthcare level by general practitioners (GPs) with specialist referrals reserved for initial evaluation of osteoporosis or in the context of complex cases or fracture liaison services (FLS). This is the case in only 16 of 28 countries surveyed. There are also wide variations in the specialties that cater to osteoporosis and metabolic bone disease and in the training of primary care physicians. All these disparities in service provision contribute to further inconsistencies in the care of patients with osteoporosis and fragility fractures.
Looking at your findings, the treatment gap has widened from 55% of women who were eligible for treatment but were left untreated in 2010 to an average of 71% in 2019. Why do you think this is and what can be done to reduce the gap?
Comparing the 27 countries included in the 2010 report to the same 27 countries in 2019, the treatment gap of osteoporosis increased in 18 countries and decreased in nine countries. Overall, the number of women at high risk who were left untreated increased from 10.6 million in 2010 to 14 million in 2019. Studies to date provide little insight into the causes underlying the substantial and increasing treatment gap. Factors that may play a role include a decline in BMD testing owing to reimbursement issues. Others point the finger at the lay press for raising awareness over the last decade of the potential side effects of bisphosphonates, the most commonly used medications. Indeed, many doctors, dentists, and patients are now more frightened of the rare but serious side effects than they are of the disease and the fractures that arise. Non-adherence to medication is also a major problem. A systematic review estimated the average cost of non-adherence to osteoporosis medications to be €28,311/patient (2020 prices), substantially more than for cardiovascular disease (€ 7,928) or gastrointestinal disease (€ 20,085), among other examples.
There is now good evidence that treatment uptake is improved by the institution of fracture liaison services (FLS). These are coordinated, multidisciplinary services that identify, diagnose, treat, and follow up patients who have sustained a fragility fracture. In a recent study, treatment uptake with FLS management increased by 76% within the first year following a major osteoporotic fracture in Swedish women. In men, the uptake more than doubled. However, a large treatment gap was still evident in men (87%) and women (63%), particularly at the extremes of age. Based on expert opinion, FLSs in hospitals were lacking in eight of the 29 countries surveyed, and approximately half of the remaining countries reported that less than 10% of hospitals had such vital programs in place.
SCOPE 2021 found other notable inadequacies in service provision that are certainly obstacles to diagnosis and treatment. In many countries, there is suboptimal availability of DXA scanners, which are used to diagnose and monitor osteoporosis. Ten countries reported having less than the estimated minimum DXA units required, and only 15 of the 28 countries that provided data, offered full reimbursement. Although a wide variety of approved medications are available for the management of osteoporosis, less than half of the countries offered full reimbursement for these medications – placing medication out of reach for some Europeans in need. The effective targeting of treatment to those at the highest risk of fracture requires an assessment of fracture risk such as FRAX. FRAX is available in 24 out of 29 countries, but guidance on the use of risk assessment within national guidelines is available only in half of the countries.
How important is a collaboration between services in creating a joined-up approach to osteoporosis care? Could health and care providers benefit from a more centralised base of resources and data?
We have seen the benefits of FLSs, which offer coordinated, multidisciplinary care for fracture patients. In addition, there is the need for high-quality management guidelines for osteoporosis in women, men, and for secondary osteoporosis, which should be consistently and widely used in clinical practice. Several countries reported incompatibilities between their recommendations for risk assessment or treatment with the actual reimbursement policy. High-quality national data are needed, including information about the burden of disease through a national fracture registry, which includes hip fractures and clinical vertebral fractures. Systems to measure and audit the quality of care provided to people with osteoporosis and associated fractures are also needed.
How could healthcare policy and practice evolve to better alleviate the burden of osteoporosis?
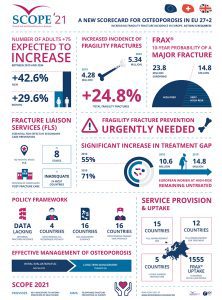
Given the projected increase in the aged population, the annual number of osteoporotic fractures across Europe (EU27 +2) is projected to rise by +24.8%; from 4.28 million in 2019 to 5.34 million in 2034. These projections indicate the urgency with which European healthcare systems must tackle the fragility fracture crisis.
Governments must mandate osteoporosis as a government-backed National Health Priority, with the implementation of an effective national action plan which addresses both policy frameworks and service provision. The latter includes providing reimbursement for approved treatments to ensure accessibility for all those at high risk of fractures and establishing adequate, accessible DXA services throughout the country. Furthermore, national guidelines, which include guidance on the use of risk assessment tools should be routinely used by clinicians. High-quality training in osteoporosis, including for primary care, and ensuring that osteoporosis is recognised with an established component of speciality training to support this. Finally, governments could support effective patient organisations that can advocate on behalf of patients and work closely with medical and research associations to improve patient care.
With SCOPE 2021, healthcare and policy professionals in Europe have a valuable tool to assess key indicators on the healthcare provision for osteoporosis and to take the appropriate action needed. As the burden of fragility fractures continues to grow and weigh heavily on healthcare systems, individuals, and their families, Europeans can no longer afford to be complacent.
References
- Kanis JA, Norton N, Harvey NC, Jacobson T, Johansson H, Lorentzon M, McCloskey EV, Willers C, Borgström F. SCOPE 2021: a new scorecard for osteoporosis in Europe. Arch Osteoporos 16, 82 (2021). doi.org/
10.1007/s11657-020-00871-9 - SCOPE 2021 resources: www.osteoporosis.foundation/scope-2021
- Willers C, Norton N, Harvey NC, Jacobson T, Johansson H, Lorentzon M, McCloskey EV, Borgström F, Kanis JA & the SCOPE review panel of IOF. Osteoporosis in Europe: A compendium of country-specific reports. Accepted for publication in Arch Osteoporosis (2022)
Professor John Kanis
Honorary President
International Osteoporosis Foundation
www.osteoporosis.foundation
https://twitter.com/iofbonehealth?ref_src=twsrc%5Egoogle%7Ctwcamp%5Eserp%7Ctwgr%5Eauthor
This article is from issue 20 of Health Europa Quarterly. Click here to get your free subscription today.






